
Rheumatic fever is an inflammatory disease that occurs following a Streptococcus pyogenes infection, such as strep throat or scarlet fever. Believed to be caused by antibody cross-reactivity that can involve the heart, joints, skin, and brain, the illness typically develops two to three weeks after a streptococcal infection. Acute rheumatic fever commonly appears in children between the ages of 6 and 15, with only 20% of first-time attacks occurring in adults. The illness is so named because of its similarity in presentation to rheumatism.

Major criteria
Group A streptococcus pyogenes has a cell wall composed of branched polymers which sometimes contain M protein that are highlyantigenic. The antibodies which the immune system generates against the M protein may cross react with cardiac myofiber protein myosin,heart muscle glycogen and smooth muscle cells of arteries, inducing cytokine release and tissue destruction. However, the only proven cross reaction is with perivascular connective tissue.[citation needed] This inflammation occurs through direct attachment of complement and Fc receptor-mediated recruitment of neutrophils and macrophages. Characteristic Aschoff bodies, composed of swollen eosinophilic collagen surrounded by lymphocytes and macrophages can be seen on light microscopy. The larger macrophages may become Aschoff giant cells. Acute rheumatic valvular lesions may also involve a cell-mediated immunity reaction as these lesions predominantly contain T-helper cells and macrophages.
 The management of acute rheumatic fever is geared toward the reduction of inflammation with anti-inflammatory medications such as aspirin or corticosteroids. Individuals with positive cultures for strep throat should also be treated with antibiotics. Aspirin is the drug of choice and should be given at high doses of 100 mg/kg/day. One should watch for side effects like gastritis and salicylate poisoning. In children and teenagers, the use of aspirin and aspirin-containing products can be associated with Reye's syndrome, a serious and potentially deadly condition. The risks, benefits and alternative treatments must always be considered when administering aspirin and aspirin-containing products in children and teenagers. Ibuprofen for pain and discomfort and corticosteroids for moderate to severe inflammatory reactions manifested by rheumatic fever should be considered in children and teenagers. Steroids are reserved for cases where there is evidence of involvement of heart. The use of steroids may prevent further scarring of tissue and may prevent development of sequelae such as mitral stenosis. Monthly injections of longacting penicillin must be given for a period of five years in patients having one attack of rheumatic fever. If there is evidence of carditis, the length of Penidure therapy may be up to 40 years. Another important cornerstone in treating rheumatic fever includes the continual use of low-dose antibiotics (such as penicillin, sulfadiazine, orerythromycin) to prevent recurrence.
The management of acute rheumatic fever is geared toward the reduction of inflammation with anti-inflammatory medications such as aspirin or corticosteroids. Individuals with positive cultures for strep throat should also be treated with antibiotics. Aspirin is the drug of choice and should be given at high doses of 100 mg/kg/day. One should watch for side effects like gastritis and salicylate poisoning. In children and teenagers, the use of aspirin and aspirin-containing products can be associated with Reye's syndrome, a serious and potentially deadly condition. The risks, benefits and alternative treatments must always be considered when administering aspirin and aspirin-containing products in children and teenagers. Ibuprofen for pain and discomfort and corticosteroids for moderate to severe inflammatory reactions manifested by rheumatic fever should be considered in children and teenagers. Steroids are reserved for cases where there is evidence of involvement of heart. The use of steroids may prevent further scarring of tissue and may prevent development of sequelae such as mitral stenosis. Monthly injections of longacting penicillin must be given for a period of five years in patients having one attack of rheumatic fever. If there is evidence of carditis, the length of Penidure therapy may be up to 40 years. Another important cornerstone in treating rheumatic fever includes the continual use of low-dose antibiotics (such as penicillin, sulfadiazine, orerythromycin) to prevent recurrence.
Patients with positive cultures for Streptococcus pyogenes should be treated with penicillin as long as allergy is not present. This treatment will not alter the course of the acute disease.
 Some patients develop significant carditis which manifests as congestive heart failure. This requires the usual treatment for heart failure: diuretics and digoxin. Unlike normal heart failure, rheumatic heart failure responds well to corticosteroids.
Some patients develop significant carditis which manifests as congestive heart failure. This requires the usual treatment for heart failure: diuretics and digoxin. Unlike normal heart failure, rheumatic heart failure responds well to corticosteroids.

Diagnosis
Major criteria
Modified Jones criteria were first published in 1944 by T. Duckett Jones, MD. They have been periodically revised by the American Heart Association in collaboration with other groups. According to revised Jones criteria, the diagnosis of rheumatic fever can be made when two of the major criteria, or one major criterion plus two minor criteria, are present along with evidence of streptococcal infection: elevated or rising antistreptolysin O titre or DNAase.Exceptions are chorea and indolent carditis, each of which by itself can indicate rheumatic fever.
 |
| most severe complication in rheumatic heart disese. |
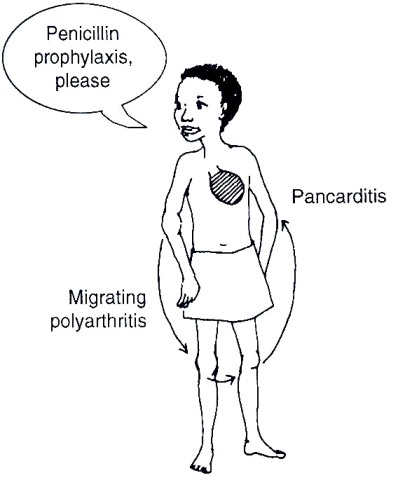
- polyarthritis: a temporary migrating inflammation of the large joints, usually starting in the legs and migrating upwards.
- Carditis: inflammation of the heart muscle which can manifest as congestive heart failure with shortness of breath, pericarditis with a rub, or a new heart murmur.
- Subcutaneous nodules: painless, firm collections of collagen fibers over bones or tendons. They commonly appear on the back of the wrist, the outside elbow, and the front of the knees.
- Erythema marginatum: a long lasting rash that begins on the trunk or arms as macules and spreads outward to form a snake like ring while clearing in the middle. This rash never starts on the face and it is made worse with heat.
- Sydenham's chorea (St. Vitus' dance): a characteristic series of rapid movements without purpose of the face and arms. This can occur very late in the disease for at least three months from onset of infection.
 |
| erythema. |

subcutaneous nodules.
Minor criteria
 |
| subcutaneous nodules. |
- Fever of 38.2–38.9 °C (101–102 °F)
- Arthralgia: Joint pain without swelling (Cannot be included if polyarthritis is present as a major symptom)
- Raised erythrocyte sedimentation rate or C reactive protein
- Leukocytosis
- ECG showing features of heart block, such as a prolonged PR interval (Cannot be included if carditis is present as a major symptom)
- First Degree AV-Block
- Previous episode of rheumatic fever or inactive heart disease
Other signs and symptoms
- Abdominal pain
- Nose bleeds
- Preceding streptococcal infection: recent scarlet fever, raised antistreptolysin 0 or other streptococcal antibody titre, or positive throat culture.
Pathophysiology
Rheumatic fever is a systemic disease affecting the peri-arteriolar connective tissue and can occur after an untreated Group A Beta hemolytic streptococcal pharyngeal infection. It is believed to be caused by antibody cross-reactivity. This cross-reactivity is a Type II hypersensitivityreaction and is termed molecular mimicry. Usually, self reactive B cells remain anergic in the periphery without T cell co-stimulation. During a Streptococcus infection, mature antigen presenting cells such as B cells present the bacterial antigen to CD4-T cells which differentiate into helper T2 cells. Helper T2 cells subsequently activate the B cells to become plasma cells and induce the production of antibodies against the cell wall of Streptococcus. However the antibodies may also react against the myocardium and joints,producing the symptoms of rheumatic fever.
In acute rheumatic fever, these lesions can be found in any layer of the heart and is hence called pancarditis. The inflammation may cause a serofibrinous pericardial exudate described as "bread-and-butter" pericarditis, which usually resolves without sequelae. Involvement of the endocardium typically results in fibrinoid necrosis and verrucae formation along the lines of closure of the left-sided heart valves. Warty projections arise from the deposition, while subendothelial lesions may induce irregular thickenings called MacCallum plaques.
Chronic rheumatic heart disease is characterized by repeated inflammation with fibrinous resolution. The cardinal anatomic changes of the valve include leaflet thickening, commissural fusion and shortening and thickening of the tendinous cords.
Prevention
Prevention of recurrence is achieved by eradicating the acute infection and prophylaxis with antibiotics. The American Heart Association recommends daily or monthly prophylaxis continue long-term, perhaps for life.

Treatment
Infection
 |
| streptococcus bacterai |
The most appropriate treatment stated in the Oxford Handbook of Clinical Medicine for rheumatic fever is benzylpenicillin.
Inflammation
Patients with significant symptoms may require corticosteroids. Salicylates are useful for pain.
Heart failure
Some patients develop significant carditis which manifests as congestive heart failure. This requires the usual treatment for heart failure: diuretics and digoxin. Unlike normal heart failure, rheumatic heart failure responds well to corticosteroids.
My little princess is so beautiful) I underwent using Dr Itua Herbal Medicine. I had a miscarriage 7 years ago. I still can’t hold back my tears when I remember that horrible period of my life. After my loss I couldn’t get back to life for a long time. I’m glad I have my husband. He gave me support I needed the most. Together we can do everything! We wanted to have kids for a really long time. We’ve gone through a lot, but if you want something badly, you’ll get it! I had to search online on how i can use herbal remedy due to my infertility then i came across Dr Itua how he cure all kind diseases and helped a lady from Kansas City to get pregnant so i contacted him on email,He gave me some guild lines to follow he also send me his herbal medicine via courier service which he instruct me on how to drink it for two weeks really i did and after 7 days of having intercourse with my husband few days later i noticed my period didn't come then i decided to go for check up i was pregnant with a baby,Dr Itua is a genuine miracle man..I've got pregnant from first attempt. We were over the moon! Our girls were born in May 2015. We've just celebrated their first birthday. Finally joy and peace came to our family.Here his Email/Whatsapp Number...+2348149277967/ drituaherbalcenter@gmail.com He cure the following...infertility Liver/kidney Inflammatory,Diabetis,Herpes Virus, Lupus, HPV, Cancer, Hiv/Aids, Hepatitis, Als, MS, Menstrual Cramp, Fribroid.
ReplyDelete